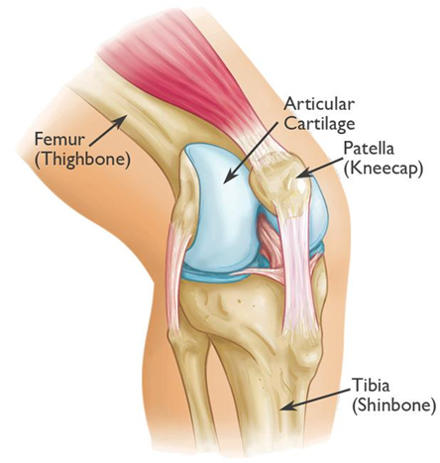
Patella and Patella Dislocation
The patella, also commonly known as the knee cap, is a mobile bone at the front of the knee. Patella or knee cap dislocation commonly occurs in the young but can affect the middle age person as well. It can either completely ‘pop’ out of its position at the front of the knee (patella dislocation), in which case it will be very obvious, or it can partially shift out of position (patella subluxation), in which case the patient will feel it ‘move out instantaneously and then back into position’.

Patella dislocation can occur because of a traumatic injury (usually during physical activity or due to an accident) or spontaneously. Those who dislocate their patella spontaneously or with minimal trauma to the knee, usually have bony structural abnormalities that predispose them to repeat patella dislocation.

Most patients with first-time traumatic dislocation will usually complain of a ‘pop’ during a traumatic injury to the knee. Patella dislocation is one of two conditions that typically present with a ‘pop’ after a twisting/pivoting injury to the knee during sports, the other common ‘popping’ knee injury being an anterior cruciate ligament (ACL) injury. There will be immediate pain and swelling of the knee as the patella ‘pops’ out of position.
The patient may notice an inability to straighten or bend the knee, also called a ‘locked’ knee. At times the knee cap will spontaneously snap back into position. In other situations, the patient will need to go to the Emergency Department to relocate the patella and ‘unlock’ the knee before the knee can comfortably bend and straighten again.
The knee may continue to swell and feel stiff for 4 to 6 weeks even after the patella is reduced in place. There may also be difficulty walking and weight-bearing on the injured leg.
Management of Acute Patella Dislocation
Fortunately, most patella dislocations do not recur, and hence most can be treated successfully with physiotherapy, with a gradual return to normal activities. If patella dislocation/subluxation recurs (recurrent patella dislocation or instability), this will then require a thorough work-up and possibly surgery to prevent further dislocations. Recurrent patella dislocations are more common in females, and in the young and active.
The usual reasons for the patella to repeatedly dislocate is because of either a bony structural abnormality of the knee, or a laxity(looseness) of the soft tissue around the knee, or both. These factors contribute to the patella being unstable, and hence repeatedly dislocate with increasing ease.
With the help of an MRI and sometimes a CT scan, the factors causing the patella to repeatedly dislocate can be determined to help guide the surgical management in patients with recurrent patella dislocation/instability.
For patients with recurrent dislocation requiring surgery, the majority can be treated with a minimally invasive key-hole surgery to recreate an important ligament (MPFL: medial patella-femoral ligament) that stabilizes the patella. MPFL reconstruction is typically done as single-day surgery under general anesthesia.
Most patients will require the use of a brace and crutches for the 1st 6 weeks after surgery, before gradually fully regaining range of motion and function by 4 to 6 months.


For patients with recurrent dislocation due to bony structural abnormality, the surgery (osteotomy) required to correct the bony structure of the knee is an open and more invasive surgery. These patients usually have bilateral knee patella instability and are young.
Overall, bony corrective osteotomy surgery is required in only a minority of patients with patella instability. Trochleoplasty and tibial tubercle osteotomy are the two common osteotomy procedures performed for patella instability.
With patella stabilization surgery, the risk of re-dislocation after surgery is significantly reduced to less than 10%.
For a more thorough understanding and evaluation of patella instability and dislocation, please contact our sports and arthroscopic surgeon, Dr Andy Wee, directly at +65 62477958.
Looking For A Reliable Knee Orthopaedic Specialist?
Fast Medical Attention, Transparent Fees
Make an appointment for comprehensive care for your knee problems!