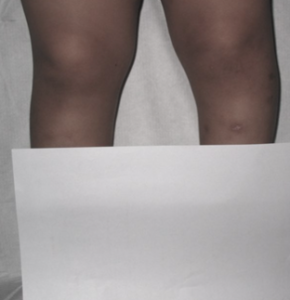
Blount’s disease is an abrupt and progressive deformity of the knee causing bowing. It can affect one or both legs. This occurs when there’s growth delay at the inner aspect of the growth plate at the knee (more specifically tibial/leg).
It is dichotomised into infantile (2 to 5 years old) and adolescent (more than 10 years old). Both demonstrate similar histological appearances of the growth plate.
What is the Cause of Blount’s Disease?
Infantile Blount’s cause is undetermined but could be due to overloading in the child with a genetic predisposition. It is seen in overweight children and early walkers.
What are the indications that it may be Blount’s as opposed to a physiological bowing?
Whereas physiologic bowing presents with a gentle curvature of the entire extremity, in Blount’s the angular deformity is abrupt and just below the knee.
A simple screen:
- Genu varum(bowing) is not considered physiological and should be suspected to be pathological if it occurs in the child older than 5
- Distance between the inner aspect of knees > 8cm
- Overweight child.
In the physical examination, the clinician looks for genu varum(bowing), flexion and internal rotation deformities. The “cover” test may be utilised to demonstrate the deformity is isolated to the proximal tibia indicating it is, in fact, a Blount’s disease.
The child exhibits an outward thrust while walking due to a resultant laxity of ligaments on that side. This also serves to worsen the stress over the growth plate.
X-rays complement physical examination and help in making the diagnosis. (Figure 2) It allows for the measurement of angles and placement in the Langenskiold Classification. (Figure 3)
This classification is useful for indicating the prognosis according to the stage. MRI is not mandatory for diagnosis but can show the extent of the physeal disruption.


Is there room for conservative treatment?
Children in early stages 1 and 2 are treated with Brace to minimise stress to the growth plate. It should be worn full-time especially when walking. It’s been found to be less useful if the child is >3 years.
When is Surgery Indicated?
Surgery is indicated in children with progressive deformity despite bracing, who are too old for bracing or present with advanced stages or high MDA.
Its aim is to restore normal growth where possible, correct mechanical axis and prevent arthritis by levelling the knee joint.
Bone cuts are made in the proximal tibia to restore the normal axis of the lower limb. This can be combined with epiphysiodesis (intentional closure of the growth plate). In some cases, bone lengthening may be required as well.
Therefore early diagnosis allows for best outcome and treatment.
What about Adolescent Blount’s?
Adolescent Blount’s is less common, and affects the femur (thigh bone) as well as the leg bone (tibia), in children >10 years of age.
There is a strong association with obesity and tends to occur on one side. It is considered pathologic and abnormal, and conservative management usually fails.
Clinical examination demonstrates obvious bowing, obesity and a LLD (Limb Length Deformity). X-rays show the relevant increase in angles affecting the knee and changes seen in the growth plate.
Treatment is always surgical, with conservative management reserved for mild cases only.
Surgical treatment options range from the intentional fusing of the growth plate on the outside (lateral physeal epiphysiodesis), to osteotomies (bone cuts) in the bones to realign the axis and a combination of both.
Looking For A Reliable Paediatric Orthopaedic Orthopaedic Specialist?
Fast Medical Attention, Transparent Fees
Make an appointment for comprehensive care for your paediatric orthopaedic problems!